en
Fonseca anamnestic index for screening Temporomandibular Disorders - reliability to discriminate muscular from intra-articular disorders.
/social-network-service/media/default/6809/fbab08d0.jpg)
44
26 min read
24 April 2025
Abstract
Background/ Objective: Fonseca anamnestic index (FAI) is a simple and quick survey used for screening the presence and severity of Temporomandibular Disorders (TMD). The presented study aimed to screen the FAI accuracy to discriminate different types of TMD: intra-articular (AD), Masticatory Muscular Disorder (MMD), or the presence of both typologies.
Methods: The existence of a pattern in the FAI based on the frequency of answers was evaluated and supported by other variables: sex, age, medical diagnosis and Visual Analog Scale of health-related quality of Life (VASLife). The non-parametric Chi-square test (𝜒2) or Fisher's exact test were used to assess the existence of associations between these variables. In the pairs of variables where such association was identified, its intensity was measured by Cramér's V Coefficient. The prediction if FAI could be a good decision tool for distinguish the type of TMD was assessed through logistic regression models (ordinal and multinomial).
Results: The higher FAI score was associated with questions related with temporomandibular joint (TMJ) pain, TMJ clicks and person anxiety. Severe cases classified by FAI are correlated with typology of Both (AD+MMD). Moreover, the female patients presented more moderate and severe cases in FAI and also correlated with the presence of AD+MMD. The logistic model showed low accuracy to distinguish the TMD typology (~70%).
Conclusion: FAI is a good initial methodology in TMD diagnosis, however integrated in a logistic regression model for distinguish the typology of TMD has proved to be insufficient. It is expected that the combination of this survey with other outcomes will make the model more accurate.
Introduction
Temporomandibular disorders (TMD) are a set of musculoskeletal and/or articular conditions that affect respectively the masticatory musculature and/or the temporomandibular joint (TMJ) complex. TMD is the most common nondental cause of orofacial pain and have a negative impact on the patient's daily life.
Epidemiologically it is known that this disease affects mainly females (70-85%) [2]. TMD present a multifactorial etiology and due to its complexity represents a real challenge for clinicians in terms of a correct diagnosis. The two main origins of pain in this region are associated with intra-articular or masticatory muscle changes. Actually, the diagnosis of TMD is largely based on the patient's symptoms, as pain in TMJ and surrounding muscles, difficulty in opening the mouth, and other complaints such as the presence of clicking in the joint, malocclusion and headaches. Clinical observation evaluates different parameters such as the presence of joint inflammation (synovitis), measurement of mouth opening and laterality of jaw movements, dental occlusion, the presence of clicks and crepitus in the joint and muscle tenderness. Definitive diagnosis is normally performed with medical imaging support, using computed tomography (CT), magnetic resonance imaging (MRI) or minimally invasive diagnostic interventions.
The Fonseca Anamnestic Index (FAI) is a TMD patient-reported questionnaire, quick and easy to administer, based in signs and symptoms with 10 questions, used in recent years to classify the severity of TMD.
The final score obtained can be interpreted using a classification table that assigns each individual one of four possible categories of severity: no TMD (0≤FAI≤15 points); mild TMD (20≤FAI≤40 points); moderate TMD (45≤FAI≤65 points) and severe TMD (70≤FAI≤100 points). However, it is unknown if the score obtained by this survey can contribute to a correct TMD diagnosis regarding three possible typologies: Articular Disorder (AD), Masticatory Muscle Disorder (MMD) or both. The aim of this study is to identify patterns in the FAI, together with the characteristics of the patients, allow us to assess the robustness of this questionnaire as an aid in the clinical diagnosis of TMD.
Methods
Study Design
A retrospective study was conducted in a private health institution in Portugal (Instituto Português da Face), including patients diagnosed with TMD from January of 2019 to March 2022. This study was approved by the Instituto Português da Face ethics committee (IPF/08/22). All enrolled patients gave their informed consent in writing, following current legislation. The inclusion criteria was: (1) age >18 years; (2); full response to FAI; (3) clinical diagnosis of TMD. The exclusion criteria included was: (1) a history of facial trauma or other orofacial disorder; (2) severe medical problems or impaired cognitive capacity; (3) pregnant or breastfeeding women. All patients were examined by the same doctor. The information was recorded and stored in a database (EUROTMJ). Confidentiality of information is ensured through anonymity. Demographic data for all patients like: sex and age was registered. As an initial diagnosis of the presence of a TMD, the patients were instructed to answer the FAI. The survey was applied in Portuguese, which is already validated in the literature, and was subsequently translated into English. The FAI is a Likert scale questionnaire based in 10 questions with three points/levels ("No", "Sometimes", "Yes") (Table S1). In FAI, answers are scored as follows: no - 0 points, sometimes - 5 points, yes - 10 points. The final score (0-100) was classified into the following categories: no TMD (0≤FAI≤15 points); mild TMD (20≤FAI≤40 points); moderate TMD (45≤FAI≤65 points) and severe TMD (70≤FAI≤100 points). Additionally, the Visual Analog Scale (VAS) has been used in the valuation of health-related quality of Life (VASLife) with the question: “If you could give a life impact score to your TMJ problem in a 0 to 10 scale, where 0 means no impact and 10 means the maximum impact possible, what would be your score?”. The identification of the type of temporomandibular disease (MMD, AD, Both) was performed by the clinician through medical evaluation and MRI to assess intra-articular derangements. To access the MMD derangements, muscle tenderness was measured using a 0-3 classification as defined in Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD).
Statistical Analysis
The initial methodology was to identify the existence of a pattern in the FAI based on the frequency of answers in each of its three levels (No; Sometimes; Yes) in the ten questions (Table S1). This analysis was supported by a descriptive study of the following variables: sex, age, medical diagnosis and score in VASLife. The mean was presented as the location measure accompanied by its standard deviation (SD) in the form mean±SD. The normality in the distributions of the FAI and VASLife (BevilaquaGrossi et al, 2006) was determined. Given the absence of normality, Spearman's correlation coefficient (𝒓𝒔) was used to determine the correlation
between the FAI and VASLife scales. The classification of the correlation was determined in accordingly with Davis. Subsequently, based on each patient's FAI score, bivariate contingency tables were created containing the absolute frequency in each of the possible combinations of categories in the following pairs of variables: TMD severity vs sex/diagnosis; diagnosis vs FAI levels for each of the items. The non-parametric Chi-square test (𝝌𝟐) and Fisher's exact test were used to assess the existence of associations between these variables. In the pairs of variables where such association was identified, its intensity was measured by Cramér's V Coefficient (𝝋𝑪). To compare more than two groups was used the non-parametric Kruskal-Wallis test and when there was statistical significance the Mann-Whitney (W) test was used for pair-wise comparison.
Finally, the extent to which the FAI could be a good decision tool for distinguish the type of TMD was assessed through logistic regression models (ordinal and multinomial). To avoid bias, the final sample (171 patients) was subdivided into two data sets: one for training (adjustment) with 70% of the information and another for testing (validation and prediction) with the remaining. The response variable considered in logistic regression models (ordinal and multinomial) was type of TMD, constituted by mutually exclusive classes (each patient is assigned to only one class), with the following ordering based on the complexity of the TMD typology: MMD<AD<Both. Moreover, the independent variables of the regression models were: FAI, SEX, Age and VASLife. The following models were considered: Model 1: TMD ~ 𝜷𝟏𝑭𝑨𝑰 + 𝜺; Model 2: TMD ~ 𝜷𝟏𝑭𝑨𝑰 + 𝜷𝟐𝑺𝑬𝑿 + 𝜺; Model 3: TMD ~ 𝜷𝟏𝑭𝑨𝑰 + 𝜷𝟐𝑺𝑬𝑿 + 𝜷𝟑𝑨𝒈𝒆 + 𝜺; Model 4: TMD ~ 𝜷𝟏𝑭𝑨𝑰 + 𝜷𝟐𝑺𝑬𝑿 + 𝜷𝟑𝑨𝒈𝒆+𝜷𝟒𝑽𝑨𝑺𝑳𝒊𝒇𝒆 + 𝜺. For the models considered, the presence of multicollinearity of the predictors was tested through the Variance Inflation Factor (VIF). In a first approach, ordinal logistic regression models were considered. If the assumption of proportional hazards by Brant is not violated the choice was ordinal logistic regression models, otherwise the multinomial logistic regression models were adopted. For this last class of models the independence of irrelevant alternatives was tested by the Hausman-McFadden test (p-values≈1). The model that presented the lowest Akaike Information Criterion(AIC) value and the highest Nagelkerke's pseudo R2 value was adopted as a selection criterion. The accuracy of the model was also presented as well as its degree of agreement expressed by Kappa coefficient (Poor<0.00; Slight:0.00-0.20; Fair:0.21-0.40; Moderate:0.41-0.60; Substantial:0.61-0.80; Almost Perfect:0.81-1.00) and classified according to Landis and Koch.
The significance level set was 5% and all statistical treatment and graphical representation was performed in the R programming language.
Results
A total of 541 patients (80% of female), with a mean age of 39.543±15.951 years, who answered the Fonseca questionnaire were included in the study. FAI score was 58.822±21.313. Initially, an assessment of the frequency of answers and mean score of the different FAI questions was performed. The items 7, 6, 10 had the highest mean score on the FAI, which reflects a higher concentration of answers at the last level of the scale (Yes) (Figure 1). In opposition, the items with the lowest mean score were 1, 9 and 2, respectively, reflected by the less frequent answers in the highest score (Yes) (Figure 1).
In second part of study, 171 patients with clinical diagnosis (between 18 and 90 years old), were included. 30 patients were diagnosed with MMD and 33 with AD and 108 with both. Patients had a mean age of 38.444±16.172 years, 140 of whom were female (82%). Female patients had a higher mean age (39.200) than male patients (35.032), although without statistical significance (Mann-Whitney (W) = 2513.500; p= 0.169).
The average pain impact on patients' lives (VASLife) was 6.525 ±2.423, with females having higher averages than males (6.781 vs 5.433, W=2579.500, p= 0.003). The global FAI mean was 60.380 ± 21.337, being differentially expressed between females and males (62.071 vs 52.742, respectively, W=2744.500, p= 0.021).
Initially, an analysis was performed between the two scales, VASLife and FAI.. A moderate positive correlation between the two scales was verified (𝑟𝑠=0.358; p<0.001), i.e. an increase in the FAI score is accompanied by an increase in the VASLife scale.
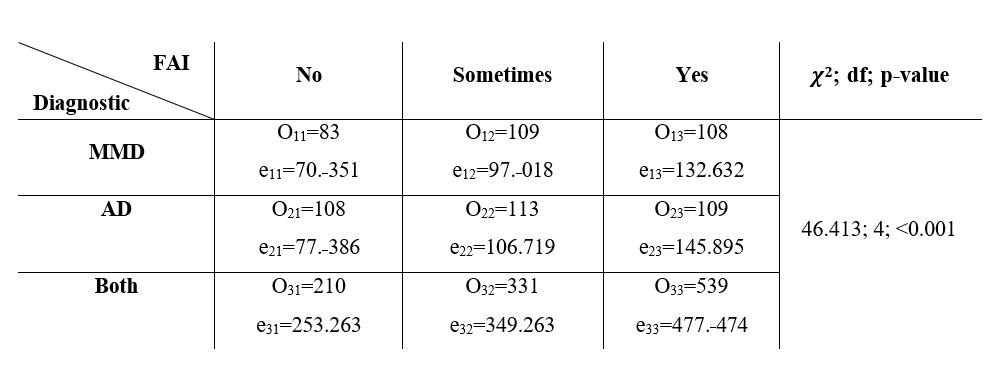
Subsequently, the existence of an association between the type of diagnosis (MMD, AD, Both) and the level of the FAI (No, Sometimes, Yes) was assessed. Once the conditions for applicability of the Chi-Square test (𝜒2), were verified, i.e. “expected values eij > 1 and 80% eij > 5”, it was determined that there was a statistically significant relationship between these variables (𝜒2 =46.413, df=4, p<0.001) (Table 1). Cramér's V coefficient assumed a value of 0.116 and is classified as moderate (𝐶𝐼𝜑𝐶95% :[0.078;0.147]). The relative frequency of diagnosis per item of the FAI at each level was then analyzed (Table S2). This results seems to indicate that: a) in MMD diagnosis the items that present higher relative frequency was the items 4,5,6 and 8; b) the AD and both diagnosis presented the higher relative frequency in items 6 and 7. Furthermore, both (MMD+AD) diagnosis presented the highest FAI scores comparatively to MMD and AD (Kruskal-Wallis chi-squared = 16.734, df = 2, p<0.001; Both vs AD, p=0.001; and Both vs MMD, p=0.019) (Figure 2).
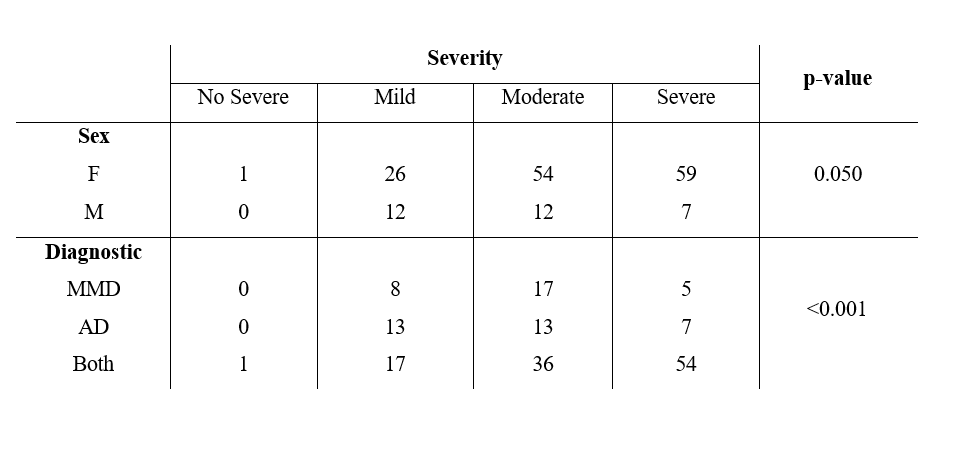
Analogously, the analysis was carried out considering the sex and diagnosis of the patient with the severity of the FAI (no severe, mild, moderate, severe). Once the conditions for the applicability of the 𝜒2 were violated, we used Fisher's exact test, which seems to indicate that there were statistically significant relationships between these pairs of variables (p=0.050; p<0.001 respectively, Table 2). Cramér's V coefficient assumed the values of 0.208 ((𝐶𝐼𝜑𝐶95% :[0.009;0.335])] and 0.245 ((𝐶𝐼𝜑𝐶95% : [0.092;0.325])) classifying the intensity as strong and very strong.
The frequency distribution of the number of diagnosed cases and the FAI score by type of TMD according to sex was then checked (Figure 3A and B). In the case of female patients there is a prevalence of diagnosis of MMD+AD (Both) (69%), while in the opposite sex AD (52%) is the most prevalent. In Figure 3B in females FAI score was significantly higher in Both diagnosis comparatively to MMD (Kruskal-Wallis chi-squared = 7.337, df = 2, p= 0.026; Both vs MMD, p=0.046), while in men this profile was not verified and it is not possible to draw the same conclusion. Finally, we sought to assess to what extent the FAI could be a good predictor of the type of TMD diagnosis using the ordinal logistic regression model. Once the absence of multicollinearity in the predictors confirmed by the VIF (FAI:1.174;SEX:1.070;AGE:1.028;VASLife:1.208), the null hypothesis of proportionality of risks was rejected in Models 1 to 4 (p-values 0.051; 0.000; 0.011; 0.010, respectively) leading to the approach by multinomial logistic regression. The predictors AGE and VASLife did not show any statistical significance (Model 3: AD:AGE p-value=0.307; Both:AGE p-value=0.357; Model 4: AD:AGE p-value=0.305; Both:AGE p-value=0.337;AD:VASLife p-value=0.783;
Both:VASLife p-value=0.125) and the choice between Models 1 and 2 was made. Analysis of deviance table revealed that both predictors in models 1 and 2 are statistically significant (Model 1: FAI, likelihood-ratio 𝜒2 =15.764, df=2, p-value=<0.001; Model 2: FAI, likelihood-ratio 𝜒2 =12.132, df=2, p-value<0.001, SEX likelihood-ratio 𝜒2 =17.694, df=2, p-value=<0.001). Since Model 2 has a lower AIC value relatively to Model 1 (196.732 vs 204.601) and higher Nagelkerke pseudo 𝑅2 (0.301 vs 0.213), this model was chosen. The accuracy of the model is 0.667 (𝐶𝐼95%:[0.580, 0.754]) and the level of agreement expressed by the Kappa coefficient is 0.230 being classified as fair [14]. In the model test the accuracy value was 0.629 (𝐶𝐼95% :[0.449, 0.785]) with a Kappa agreement level of 0.187. The Figure 3C represents the adjusted logistic model.
The adjusted Model 2 can be expressed by the following set of equations:

Discussion
TMD continue to represent a clinical challenge in diagnosis due to complex muscle and intra-articular involvement. Thus, a precise diagnosis of TMD is crucial and has been the object of a large number of studies.
The RDC/TMD classification continues to be the most widely used in clinical practice, contributing significantly to a standardization of diagnosis. However, at a practical level, it has implementation disadvantages, being time-consuming, difficult in data collection and requiring extensive clinical experience. On the other hand, FAI is a simple questionnaire to implement and is a useful initial tool to distinguish the presence of a TMD and the degree of severity. This tool has been the subject of study in various scientific studies. However, the accuracy of FAI to distinguish the possible origin of TMD, muscular or intra-articular, is still unknown. Thus, this study aimed to identify the behavior of the FAI in a set of patients diagnosed with different TMD.
Primarily we found that the items relatively to clicks in TMJ (item 7), pain in TMJ area (item 6) and muscle surrounding (item 3) are among the biggest contributors to higher values on the FAI . Indeed, pain seems to have a strong impact on FAI, corroborated by the moderate correlation of FAI with the VASLife scale.
Interestingly, being an anxious person can also be crucial for high FAI scores (item 10). On the other hand, the difficulty in items related to mandibular movements, either laterally or vertically, as well as the difficulty in touching the teeth were the least determinant factors (items 2, 9 and 1). Importantly, it has also been shown that higher FAI scores are correlated with a more complex diagnosis with the simultaneous presence of muscle and intra-articular changes (Both). In fact, it is possible to verify a greater number of moderate and severe cases of the FAI, when muscular changes are verified simultaneously with intra-articular alterations.
Interestingly in MMD diagnosis was found a pattern of higher relative frequency in the items related with pain (headache, neck pain and TMJ pain) and parafunctional habits (clenching or griding). On other hand, in AD and Both was verified a higher predominantly of positive answers in items related with pain and noise in TMJ area. This results, showed an alteration in higher relative frequency of FAI items when are present intra-articular derangements. At the same time, a different distribution of severity of cases in females and males was demonstrated. In females, MMD and MMD+AD were the TMD types with the lowest and highest FAI scores, respectively. In addition, there was a higher distribution of cases with both diagnoses in females. This trend was not equally demonstrated in males. Previous studies have pointed that female sex has a higher prevalence of TMD, around 80%. Although not entirely certain, hormonal imbalance in females may be related to increased susceptibility to TMD. Beyond these data, this study also showed that there is a growing trend towards more severe cases in females. A logistic model was conducted and following conclusions were drawn: (i) there is a higher probability of a patient being diagnosed with MMD, although low, have lower FAI final scores; (ii) the probability of a patient being diagnosed with AD with low FAI scores is much higher in men compared to women, a difference that is attenuated as FAI scores increase; (iii) when a patient is diagnosed with both AD and MMD simultaneously, the FAI scores show an increasing behavior, which is identical in both genders (parallel lines).
However, the present model with FAI as predictor showed an accuracy <70%, which means that for every 100 diagnoses made, at most, 70 are expected to be correctly classified. In clinical terms, a higher accuracy is desirable. Additionally, the number of diagnoses between the three groups has different values, with the MMD+AD (107) three times higher compared to the other diagnoses (~30). In addition, the number of final diagnoses (171) represents around 32% of the total number of records (539). The authors consider that a higher number of cases with final diagnosis may allow a better illustration of the role of FAI in the distinction of disease typology.
In conclusion, FAI is an important tool in the diagnosis of TMD, however a more complex model is needed to more accurately distinguish the type of TMD. In the future, it is expected that other complementary measures and scales will be incorporated to strengthen the model. This study also demonstrated a differential behavior of the FAI between the two sexes. Thus, clinicians should take sex into consideration when using this tool.
Authors: Ricardo S. João, Henrique J. Cardoso, David Sanz, David F. Ângelo
References:
- Li DTS and Leung YY. Temporomandibular Disorders: Current Concepts and Controversies in Diagnosis and Management. Diagnostics (Basel, Switzerland), 2021; 11(3): 459.10.3390/diagnostics11030459
- Bueno CH, Pereira DD, Pattussi MP, et al. Gender differences in temporomandibular disorders in adult populational studies: A systematic review and meta-analysis. J Oral Rehabil, 2018; 45(9): 720-729.10.1111/joor.12661
- Sharma S, Gupta DS, Pal US, et al. Etiological factors of temporomandibular joint disorders. National journal of maxillofacial surgery, 2011; 2(2): 116-119. 10.4103/0975-5950.94463
- Schiffman E, Ohrbach R, Truelove E, et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J Oral Facial Pain Headache, 2014; 28(1): 6-27. 10.11607/jop.1151
- Bevilaqua-Grossi D, Chaves TC, de Oliveira AS, et al. Anamnestic index severity and signs and symptoms of TMD. Cranio, 2006; 24(2): 112-8. 10.1179/crn.2006.018
- Berni KC, Dibai-Filho AV, and Rodrigues-Bigaton D. Accuracy of the Fonseca anamnestic index in the identification of myogenous temporomandibular disorder in female community cases. J Bodyw Mov Ther, 2015; 19(3): 404-9. 10.1016/j.jbmt.2014.08.001
- Stasiak G, Maracci LM, de Oliveira Chami V, et al. TMD diagnosis: Sensitivity and specificity of the Fonseca Anamnestic Index. CRANIO®, 2020: 1-5. 10.1080/08869634.2020.1839724
- Sánchez-Torrelo CM, Zagalaz-Anula N, Alonso-Royo R, et al. Transcultural Adaptation and Validation of the Fonseca Anamnestic Index in a Spanish Population with Temporomandibular Disorders. Journal of Clinical Medicine, 2020; 9(10): 3230.
- Campos JA, Carrascosa AC, Bonafé FS, et al. Severity of temporomandibular disorders in women: validity and reliability of the Fonseca Anamnestic Index. Braz Oral Res, 2014; 28: 16-21.10.1590/s1806-83242013005000026
- Institute of Medicine (US) Council on Health Care Technology; Mosteller F, Falotico-Taylor J, editors. Quality of Life and Technology Assessment: Monograph of the Council on Health Care Technology. Washington (DC): National Academies Press (US); 1989. 6, Assessing Quality of Life: Measures and Utility. Available from: https://www.ncbi.nlm.nih.gov/books/NBK235120/.
- Schiffman EL, Ohrbach R, Truelove EL, et al. The Research Diagnostic Criteria for Temporomandibular Disorders. V: methods used to establish and validate revised Axis I diagnostic algorithms. J Orofac Pain, 2010; 24(1): 63-78.
- Davis JA, Elementary survey analysis. 1971, Englewood Cliffs, N.J.: Prentice-Hall. Hosmer DW and Lemeshow S, Applied Logistic Regression. 2004: Wiley.
- Landis JR and Koch GG. The measurement of observer agreement for categorical data. Biometrics, 1977; 33(1): 159-74.
- R Core Team (2018). R: A language and environment for statistical computing. R Foundation for Statistical Computing V, Austria. Available online at https://www.R-project.org/.
- Akoglu H. User's guide to correlation coefficients. Turkish journal of emergency medicine, 2018; 18(3): 91-93. 10.1016/j.tjem.2018.08.001
- Schmitter M, Ohlmann B, John MT, et al. Research Diagnostic Criteria for Temporomandibular Disorders: A Calibration and Reliability Study. CRANIO®, 2005; 23(3): 212-218.10.1179/crn.2005.030
- Look JO, Schiffman EL, Truelove EL, et al. Reliability and validity of Axis I of the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) with proposed revisions*. Journal of Oral Rehabilitation, 2010; 37(10): 744-759. https://doi.org/10.1111/j.1365-2842.2010.02121.x
- Hasanain F, Durham J, Moufti A, et al. Adapting the diagnostic definitions of the RDC/TMD to routine Clinical practice: A feasibility study. Journal of Dentistry, 2009; 37(12): 955-962. https://doi.org/10.1016/j.jdent.2009.08.001
- Anderson GC, Gonzalez YM, Ohrbach R, et al. The Research Diagnostic Criteria for Temporomandibular Disorders. VI: future directions. Journal of orofacial pain, 2010; 24(1): 79-88.
- Janal MN, Raphael KG, Nayak S, et al. Prevalence of myofascial temporomandibular disorder in US community women. J Oral Rehabil, 2008; 35(11): 801-9. 10.1111/j.1365-2842.2008.01854.x
- Berger M, Szalewski L, Bakalczuk M, et al. Association between estrogen levels and temporomandibular disorders: a systematic literature review. Przeglad menopauzalny = Menopause review, 2015; 14(4): 260-270. 10.5114/pm.2015.56538