en
Determination of Relative Humidity in the Operative Field with Absolute, Modified, and Relative Isolation – Pilot Study
/social-network-service/media/default/102325/d3b0565f.png)
10
21 min read
02 June 2025
Machine translation
Original article is written in PT language (link to read it).
Summary
Objective: To determine the relative humidity (RH) of the air at the level of the incisal edge of the upper central incisors under different techniques of field isolation.
Material and Methods: RH measurements were performed with a digital thermo-hygrometer. Four patients were selected and subjected to three different isolation techniques: 1-absolute isolation; 2-modified isolation; 3-relative isolation. In the modified and relative isolation techniques, suction devices were also placed using a compressor and a vacuum pump to verify their influence on RH. After isolation, the hygrometer was positioned at the level of the incisal edge of the upper central incisors, and RH measurements were recorded and averages calculated.
Results: The RH of the environment on the day of measurements was 31%. The measurements with relative isolation showed an average of 98%. The use of suction reduced the RH values to 86% with a compressor and 69% with a vacuum pump. The measurements taken with modified isolation showed values ranging from 31% to 95%, depending on the use of suction systems, while those obtained under absolute isolation showed an average value of 33%.
Conclusions: The measurements demonstrate that the UR is almost completely saturated at the level of upper central incisors with relative isolation, while the values obtained with absolute isolation show that it is truly absolute, providing the best conditions for clinical procedures.
Introduction
Absolute isolation is a technique that dates back to 1864, when the dentist Sanford Christie Barnum presented it at the New York Dental Society as a possibility for use in the restorative techniques of the time. This occurred long before the development of adhesion and current techniques and materials, which determine the need for its use in restorative procedures.
Endodontics is probably the dental specialty that most utilizes absolute isolation. The rubber dam serves as a physical barrier that minimizes contamination of the root canal system by microorganisms from the oral environment and also protects the oral cavity and the patient's respiratory tract from objects and chemical substances.
Research has shown that adhesive restorative procedures are sensitive to the conditions of the oral environment, such as humidity and the presence of contaminants like blood, saliva, gingival fluid, and lubricants from handpieces. Air humidity is a constant factor in dental practice, not only due to the presence of oral fluids but also because of the air exhaled by the patient, which causes high humidity in the oral cavity, approaching 100%. Therefore, adequate isolation of the operating field is essential for the long-term success of adhesive restorations.
It is known that absolute isolation facilitates and increases the effectiveness of various clinical procedures, as it provides a dry operating field free from contamination by fluids and microorganisms, improves the visual field, retracts soft tissues, protects the patient, the operator, and the assistant, making the treatment safer and more effective.
Studies evaluating the success and failure rates of indirect ceramic restorations of the inlay type cemented with different adhesive systems and cements reveal a failure rate of only 4% after a follow-up of 4 years when cementation is performed under absolute isolation. On the other hand, direct restorations made with composite resin under absolute isolation in class I and II cavities show success rates of 75% and 64% respectively after 17 and 22 years of follow-up.
Browet and Gerdolle (2017) suggest that there are three fundamental points that result in the success of absolute isolation: the materials, the strategy, and the technique. These points must be fully understood and correctly applied to achieve the highest quality of isolation.
However, despite all the benefits, many professionals do not routinely use absolute isolation in their clinical practice when performing adhesive procedures, leading them to primarily work with relative isolation of the operating field. The main reasons reported for not using absolute isolation are technical difficulty, clinical time consumption, and the difficulty of achieving adequate interproximal contacts when performing direct restorations.
By using alternative means that offer partial isolation such as lip retractors, cotton rolls, and saliva ejectors, it is possible to control the direct contact of saliva with the dental surfaces to be restored, without taking into account the relative humidity of the air generated by the patient's breathing, a determining factor in the adhesive protocol.
The objective of this work was to determine the relative humidity of the air at the level of the incisal edge of the upper central incisors under absolute isolation with a rubber dam, relative isolation with a mouth opener, and modified isolation technique.
Materials and methods
For the humidity analysis, a digital thermo-hygrometer (DIEHL Thermotron Hygro) was used, an instrument that measures the temperature and relative humidity of the ambient air.
Different measurements of the relative humidity of the air in the office environment were taken, to then compare it with the relative humidity of the air at the level of the upper central incisors of four patients subjected to different types of operative field isolation.
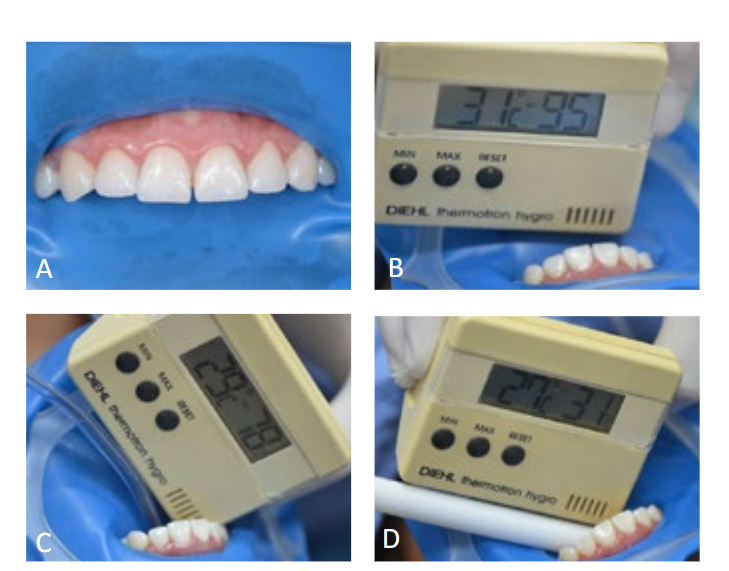
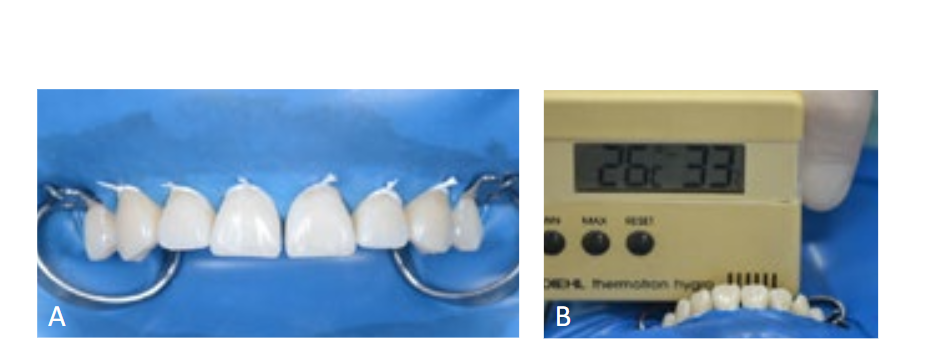
After positioning the patient in the dental chair, three different isolation techniques were performed: 1-relative isolation with a lip retractor and cotton rolls (Image 1A); 2-modified isolation with a rubber dam and an enlarged opening for all upper incisors (Image 2A); 3-absolute isolation with clamps and a rubber dam (Image 3A). In the modified and relative isolation techniques, suction devices were also placed using a compressor and a vacuum pump (high power), to verify their influence on the relative humidity.

After the isolation was performed, the digital hygrometer was positioned at the level of the incisal edge of the upper central incisors and the relative humidity values were recorded. A total of 12 measurements were obtained, from which the averages were calculated to verify the results.
Results
The average values found for each clinical situation are described in Table 1.
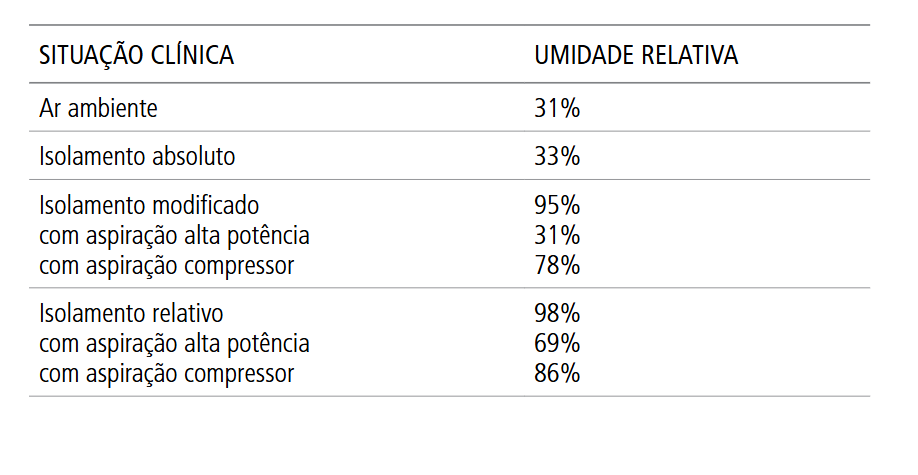
The relative humidity of the office environment on the day of the measurements was 31%. The results obtained from measurements taken in the mouth with relative isolation showed an average value of 98%, demonstrating that the air at this level, solely from the patient's breathing, was almost completely saturated with moisture (Image 1B). The use of suction reduced the relative humidity values to 86% with a compressor and 69% with a vacuum pump (Images 1C and 1D).
The measurements taken with modified isolation showed values that varied from 31% to 95% relative humidity, depending on the use of auxiliary suction systems (Images 2B, 2C, and 2D).
The measurements obtained under absolute isolation of the operative field showed an average value of 33% relative humidity, with these results being very close to the relative humidity value of the environment (Image 3B).
Discussion
The present study evaluated the relative humidity in the region of upper incisors subjected to different techniques of operative field isolation and showed that absolute isolation and modified isolation associated with the use of high-power suction provided a relative humidity close to that found in the ambient air.
Adhesive procedures are essential for most restorative protocols used in modern dentistry. Different techniques are used to establish good adhesion between restorative materials and the dental substrate, in order to prevent the formation of gaps and microleakage, reducing clinical problems and promoting greater predictability in treatment. Significant efforts have been made to develop restorative materials that adequately adhere to dentin in the oral environment without complicated clinical procedures.
The basic mechanism of adhesion to enamel and dentin is essentially an exchange process, which involves the replacement of mineral removed from the hard dental tissue with resin monomers, which, after polymerization, become micromechanically interconnected to the created porosities. In the oral environment, water is always present and can have a deleterious effect on polymerization, potentially affecting adhesive restorative processes in various ways, both before and after polymerization.
It is known that in addition to moisture, fluids such as saliva, blood, and other contaminants are cited as causes of failures in the adhesion process. Common methods of moisture control include rubber dam and cotton rolls combined with suction. The rubber dam provides an ideal dry operating field while the procedure is performed, and this isolation is widely considered to reduce failures and increase the longevity of the treatment. Rubber dams also control cross-contamination, reducing microbial aerosol during cavity preparation and providing a barrier to potential spread of infectious diseases in the dental office environment.
The analysis of the moisture conditions under which adhesive procedures will be performed is extremely important. In many clinical situations, where the dentist must execute or cement restorations very close to soft tissues or even within the gingival sulcus, absolute isolation represents a true challenge. However, it is also known that this will undoubtedly provide the ideal working conditions. Therefore, the knowledge, materials, and necessary training are essential to achieve absolute isolation of the operative field that provides these conditions.
The success of adhesion is challenged by several factors and can be influenced by the type and surface treatment given to the substrate, the type and treatment given to the restorative material, the correct execution of the technique, as well as the type and quality of the adhesive or cementation system used. In general, adhesive systems are highly sensitive to extrinsic moisture to dentin, resulting in very low adhesive strength values in high humidity, as demonstrated in several laboratory studies conducted to evaluate the influence of relative humidity on adhesive procedures. Plasmans et al. (1993) evaluated in vitro the moisture sensitivity of the adhesive strength of four adhesive systems. There was a significant difference for all adhesives when comparing high (95%) and low humidity (40%), with the lowest adhesion values at high humidity.
Miyazaki et al. (2001) and Chiba et al. (2004) investigated the influence of temperature and relative humidity on the adhesion to dentin of different adhesive systems in vitro. The authors observed that the higher the humidity, the lower the adhesive strength to dentin. When the specimens were subjected to a relative humidity of 95%, the adhesion of all evaluated systems significantly decreased. On the other hand, temperature did not significantly influence adhesion. These results suggest that extrinsic moisture derived from the oral cavity, when above a critical level, can negatively affect adhesion to dentin.
A literature review investigated the results of laboratory studies on the influence of temperature and relative humidity on adhesion to enamel and dentin. It was observed that humidity is an important variable during adhesive procedures, especially when testing the adhesive strength of materials in vitro with the intention of simulating in vivo conditions. Most studies demonstrated the influence of humidity on adhesion to dental tissues, but no study adequately explained this influence on the physical-mechanical processes occurring at the interface. Understanding the mechanism of adhesive failure in high humidity is essential for developing rational strategies to enhance performance and confidence in the use of adhesives where these conditions are encountered. However, the authors emphasize that the relationship between evidence of clinical performance and in vitro studies that evaluate an isolated property is problematic, but conclude that the use of the rubber dam remains essential, even if it does not eliminate the problem of high humidity in the treatment environment.
In addition to relative isolation with cotton rolls and mouth retractors, other devices have been evaluated for controlling moisture in the oral environment as an alternative to absolute isolation. Kameyama et al. (2011) assessed in patients the effect of two intraoral vacuum devices (Isolite i2 and Coolex) on temperature and relative humidity, compared to absolute isolation with a rubber dam and no isolation. The relative humidity and temperature were measured in the lower molar region by a digital device before and after the placement of the devices. The relative humidity in the absence of absolute isolation showed humidity values close to 100%, as in the present study. When using the rubber dam isolation and the tested devices, the humidity became close to that detected in the ambient air. The authors concluded that the three isolation methods tested effectively reduced the relative humidity of the operative field, improving the conditions of the environment for adhesive restorations.
Raskin et al. (2000) conducted a study comparing the clinical performance of class I and II posterior composite restorations performed with and without absolute isolation. The patients were followed for a total period of 10 years, and no significant differences were observed for the clinical criteria evaluated when using absolute or relative isolation. The authors concluded that the clinical behavior of composite restorations in posterior teeth performed correctly using effective isolation with cotton rolls and suction was not different from the behavior of restorations performed under absolute isolation with a rubber dam.
Daudt et al. (2013) evaluated the clinical performance of direct composite restorations in non-cariogenic cervical lesions performed under absolute isolation and under relative isolation with cotton rolls. A total of 62 patients were evaluated, and it was observed that the type of isolation did not influence the performance of class V composite restorations after 1 year of follow-up.
Saraiva et al. (2015) evaluated the temperature and relative humidity in anterior and posterior intraoral sites and their effects on the adhesive strength in dentin of two-step adhesive systems. The temperature and relative humidity in the molar region were higher (27ºC and 90.79%) compared to the incisor region (26ºC and 84.84%). However, these differences did not affect the immediate adhesive strength of the evaluated adhesive systems.
Although the results of clinical trials involving the performance of composite resin restorations do not show a substantial difference between absolute isolation and relative isolation with cotton rolls, these studies are scarce, and both in vivo and in vitro research results have indicated that there is an influence of the environment on the adhesive strength of restorative materials, on marginal microleakage, and on the polymerization shrinkage of composite resins. Therefore, it is preferable to avoid performing adhesive procedures in the absence of some isolation technique to maintain a dry field.
In addition to direct restorations, which have been widely investigated, another clinical condition in which relative humidity can influence adhesion is in adhesive cementation procedures for indirect resin or ceramic restorations. However, there is a scarcity of studies in the literature that evaluate the influence of the moisture in the environment on the success of cementing these pieces. The clinical criteria and the professional's experience will be crucial in diagnosing whether cementation under absolute isolation of the operating field is possible and viable or if it will represent a greater risk than a benefit.
The use of absolute isolation with a rubber dam still proves favorable for the optimal performance of adhesive procedures, confirming the traditional recommendation for its use to achieve optimal working conditions. Controlled and long-term clinical trials should be conducted in order to elucidate the real influence of the relative humidity of the operating field on adhesive procedures in current dentistry.
Conclusion
The measurements reported in this work demonstrate that the relative humidity of the air is almost completely saturated at the level of the incisal edge of a maxillary central incisor with relative isolation of the operative field. Considering that this is the region where relative isolation would have its best function, one should reflect on what the condition and control would be in other oral regions. The values obtained with absolute isolation of the operative field demonstrate that it is truly absolute, providing the best conditions for clinical procedures. Each clinical case should be evaluated individually to determine if it is possible and feasible to achieve total isolation of the dental structure for better adhesion.
Nicolas Andres Caviglia, Oscar Arauco Urzagaste, Patrícia Correia de Siqueira, Rafael de Almeida Decurcio, Daniel de Almeida Decurcio
References:
- Abrams RA, Drake CW, Segal H. Dr. Sanford C. Barnum and the Invention of the Rubber Dam. Gen Dent. 1982; 30(4):320-2.
- Malmberg L, Björkne AE, Bergenholtz G. Establishment and maintenance of asepsis in endodontics - a review of the literature. Acta Odontol Escand. 2016; 74(6):431-5.
- Kameyama A, Asami M, Noro A, Abo H, Hirai Y, Tsunoda M. The effects of three dry-field techniques on intraoral temperature and relative humidity. J Am Dent Assoc. 2011; 142(3):274-80.
- Plasmans PJJM, Reukers EAJ, Vollenbrock-Kuipers L, Vollenbrock HR. Air humidity: a detrimental factor in dentine adhesion. J Dent. 1993; 21:228-233.
- Daudt E, Lopes GC, Vieira LCC. Does Operatory Field Isolation Influence the Performance of Direct Adhesive Restorations? J Adhes Dent. 2013; 15:27-32.
- Krämer N, Ebert J, Petschelt A, Frankenberger R. Ceramic Inlays Bonded With Two Adhesives After 4 Years. Dent Mater. 2006; 22(1):13-21.
- Ferracane JL. Resin-based Composite Performance: Are There Some Things We Can’t Predict? Dent Mater. 2013; 29(1):51-8.
- Browet S, Gerdolle D. Precision and Security in restorative dentistry: the synergy of isolation and magnification. Int J Esthet Dent. 2017; 12(2):172-185.
- Rau PJ, Pioch T, Staehle HJ, Döfer CE. Influence of the Rubber Dam on Proximal Contact Strengths. Oper Dent. 2006; 31(2):171-5.
- Jacquot B, Durand JC, Farge P, Valcarcel J, Périère DD, Cuisinier F. Influence of Temperature and Relative Humidity on Dentin and Enamel Bonding: A Critical Review of the Literature-Part 1: Laboratory Studies. J Adhes Dent. 2012; 14(5):433-46.
- Chiba Y, Miyazaki M, Rikuta A, Moore BK. Influence of Environmental Conditions on Dentin Bond Strengths of One-application Adhesive System. Oper Dent. 2004; 29(5):554-559.
- Raskin A, Setcos JC, Vreven J, Wilson NHF. Influence of the isolation method on the 10-year clinical behaviour of posterior resin composite restorations. Clin Oral Invest. 2000; 4:148-152.
- Cochran MA, Miller CH, Sheldrake MA. The efficacy of the rubber dam as a barrier to the spread of microorganisms during dental treatment. J Am Dent Assoc. 1989; 119:141–144.
- Miyazaki M, Rikuta A, Tsubota K, Yunoki I, Onose H. Influence of environmental conditions on dentin bond strengths of recently developed dentin bonding systems. J Oral Sci. 2001; 43(1):35-40.
- Saraiva LO, Aguiar TR, Costa L, Cavalcanti AN, Giannini M, Mathias P. Influence of Intraoral Temperature and Relative Humidity on the Dentin Bond Strength: An in Situ Study. J Esthet Restor Dent. 2015; 27(2):92-9.
- Knight GT, Berry TG, Barghi N, Burns TR. Effects of two methods of moisture control on marginal microleakage between resin composite and etched enamel: a clinical study. Int J Prosthodont. 1993; 6(5):475-479.
- Charlton DG. Effect of humidity on the volumetric polymerization shrinkage of resin restorative materials. Gen Dent. 2006; 54(2):113-116.